

Arthritis of the Knee
The Problem
There are two main types of arthritis that many people ultimately suffer from usually after they are in their 50s or beyond. Degenerative arthritis, overwhelmingly the most common, is a breakdown of the cartilage in a joint because the genetic code does not account for enough repair and maintenance of the cartilage in the joint, which is normally alive, dynamic tissue. Imagine an abandoned house that never gets painted and the roof falls apart, the window shutters dangle and perhaps the windows themselves are broken. Another type of arthritis, inflammatory, includes relatively small numbers of people by comparison afflicted with rheumatoid arthritis. With RA, antibodies are made by attacking one’s own body, setting off an inflammatory response. Gout is also a fairly common inflammatory arthritic disease. This is a poorly understood common ailment wherein crystals of urate are engulfed by WBCs that release caustic enzymes into the joints.
There has been a tremendous increase in the number of people needing treatment for painful arthritis of the knees in particular. There has been a parallel between excessive weight gain (obesity) and patients having knee pain from arthritis. This has been termed the “obesity tsunami.” It has become an international health issue for which little direction has yet come about. At the same time, a huge percentage of the population has reached the age where one would naturally develop some arthritis anyway and accompanying this, there seems to be a less tolerant society for living with discomfort despite becoming less active naturally as one ages. Interestingly, studies have shown that patients who undergo knee replacement for arthritis do not become more active and do not lose weight afterward. At least 60 to 70% of these people in the United States are at retirement age, i.e., probably not very productive, when they end up having a joint replacement. There are alternatives for many people who are having a knee joint replacement.

Treatment Options
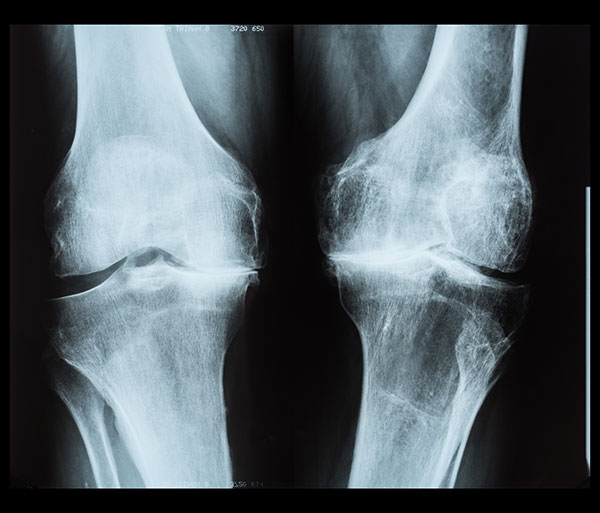
Once the doctor has examined your knee and x-rayed it (preferably weight-bearing) to clarify the cartilage thickness if there is residual cartilage in the joint, then he can help you work on weight reduction if it is feasible. This is usually most successful only in very dedicated patients and in those who are willing and physically able to take appetite-suppressant medication. Appetite-suppressant protocols seem to be the most effective while exercise contributes to the overall physical fitness of the person and the reduction of carbohydrate consumption (decrease volume of bread, pasta, rice, potatoes, sweetened drinks, and confections such as cakes and pastries, and candy).
Non-steroidal anti-inflammatory medication (NSAIDs) are the mainstay for the treatment of degenerative arthritis throughout the body, and they are also used in conjunction with cortisone, disease-modifying drugs such as Enbrel, and methotrexate in the management of autoimmune (rheumatoid) arthritis. NSAIDs were derived from analysis of the chemical pathway of aspirin which is apparently extracted from tea made from willow bark by American Indians. Aspirin in large quantities, however, causes ringing in the ears, gastritis, ulcers, and can affect one's kidneys as well. The NSAIDs derived from this chemical pathway mostly in a satisfactory, safe form, really began with ibuprofen in the late 1960s. These medicines do not cross the blood-brain barrier, i.e., they are affecting the tissue, not the brain, and pain relief comes by decreasing inflammation and cutting down on painful chemical pathways in the joint tissue. One of the problems we have with NSAIDs or with any medication is just getting the patient to take it. Studies have shown that people are unreliable and uncooperative in taking medication and the least frequent medication is taken substantially more often than medication requiring frequent dosing. Most patients can tolerate the NSAIDs without side effects as long as they have normal kidney function and do not have a true allergy to NSAIDs (rash, shortness of breath, or throat swelling) or a history of a definite ulcer or severe esophagitis. One can tell within about four to six weeks whether they are going to get substantial benefits and will be able to live comfortably with NSAIDs. These have to be taken on an ongoing basis because arthritis cannot be stopped, and we cannot roll the clock backward and generate new cartilage.
Short-term relief which can be very rapid in onset is derived from injecting cortisone into the knee joint after withdrawing any excessive joint fluid off with a large-bore needle. This usually works very well for a short time, but because of side effects and calcium metabolism, there is a general standard of limiting these to three or four per year.
Hyaluronic acid injections, a chemical originally derived in large quantity from rooster comb but now created in a laboratory in higher concentration, have benefited some people. This is expensive and has not been proven to be any better than just getting a cortisone injection periodically, which is much less expensive. HA is also not better than taking the NSAID, though it can be used in a person who is not allergic to it and in a person who cannot otherwise take NSAIDs. I consider HA to be at the very back of the table because of the expense and the lack of predictable benefits for the majority of people.
A famous orthopedic article written over 50 years ago by Dr. Blount was, “Don't Throw Away the Cane.” This is a very important potential aid to reduction in discomfort of the knee since proper use of a cane in the opposite hand of a person with arthritis predominantly in one knee reduces the weight across the knee by about 50% while walking. Unfortunately, we live in a very appearance-conscious society and an uncooperative society wherein almost no one is willing to use a cane- they just want something “fixed.”
Twenty-five to 50 pounds weight loss or more may decrease a person’s pain enough or eliminate it altogether. The alternative of weight-reduction surgery almost never results in more than 110 pounds of weight loss. This type of surgical treatment is offered by general surgeons and not orthopaedists (see note below). After weight loss surgery, some people become intolerant of NSAIDs, the mainstay in pain relief from arthritis!
Note: These are basically surgical procedures for people with major self-control problems because they are basically preventing a person from overeating, restricting the stomach volume, and diverting some of the food faster so that it is ingested is not absorbed depending on the procedure. A lot of the weight loss that occurs is actually from a large amount of fat that is cut out of the person at the time of the surgery in diversion-type surgery as opposed to stomach banding-type procedures.
Joint Replacement
For the person who cannot take anti-inflammatory medications or for whom those medications have not been successful with or without an occasional cortisone injection and/or the use of a cane, joint replacement is a good option. Over the years, orthopaedists have found that regardless of the joint being worked on- knee, hip, ankle, or finger joint, etc., the closer we reproduce the normal contour of the joint with the implant, the better the results are, allowing the most motion while avoiding a situation wherein implants are shaken loose. Joint replacement benefits a patient because the technique of insertion of the implant involves cutting thousands of nerve endings going to the joint and then covering the joint surface with high-density polyethylene on one side and cobalt- chrome-molybdenum on the other. This is akin to a dentist crowning a tooth. For most people, these components do not cause an inflammatory response in the body, and they are very durable. If implanted properly, joint replacement surgery should give a result lasting 25 years or more. There is a hesitancy to put artificial joint surfaces in young people under 50 unless they have tremendous arthritis throughout their body. Many people ignore the activity restrictions that are recommended to prevent implants from shaking loose. Jogging and routine exercise are very acceptable as is cycling. Activities that involve pounding, kicking, and forceful pivoting such as soccer or football would have a greater chance of loosening an implant.
Total knee replacement came into being in the 1960s. There were no sophisticated cutting jigs until probably about the early 1980s or so and total knee replacement was being done free-handed, or as we would say, by “eyeballing,” thus the better carpenter or perhaps the surgeon doing more volume could anticipate better results.
Partial knee replacement was invented by Dr. Marmor in Los Angeles in about 1970. Though the results were good, they did not gain wide acceptance. When jigs were introduced along with improvements in the metals and the plastics being used and even improvements in the bone cement being used in anchoring an implant, an increased volume of knee replacements was offered in conjunction with an increase in the number of people presenting with degenerative arthritis.
Total knee replacement can be expected to achieve complete satisfaction for a patient 83% of the time according to carefully-performed recent patient outcome studies. Partial-knee replacement using mobile-bearing or fixed-bearing implants tends to achieve better outcome assessment by the patient at 90% satisfaction. Patients who have had a total knee replacement on one side and a partial knee on the other tend to prefer the partial-knee replacement side. In Europe, beginning with Great Britain, a huge number of partial-knee replacements have been done over the years with very good results. This trend in doing partial knees has not been followed in the United States except by a few select surgeons across the country largely because of two unfortunate interrelated facts: 1) The United States has a very bad legal system and doctors, particularly surgeons and obstetricians, spend an awful lot of time and effort and money trying to thwart frivolous lawsuits at an enormous cost to society. 2) Tied to this was an unfortunate article in JBJS 1989 written by Drs. Stuart Kozinn and Richard Scott at the Brigham and Women’s Hospital in Boston. In my opinion, the incorrect information provided by these doctors has been responsible for enormous surgical blood loss and the need for transfusion, reduced mobility, increased hospital costs, and tremendous negative impact on our environment because of the energy expended on waste products that were created in formation and utilization of total knee rather than partial-knee replacement. Dr. Scott felt that the criteria for partial knee limited its use to only about 5% of people with knee arthritis. It turns out this is blatantly untrue, but it took others to prove this at substantial medicolegal risk in doing so. The orthopaedists very active in this area of research in the last 25 years in Indiana, Ohio, and Tennessee have demonstrated that over 50% (half) or more of the patients presenting with degenerative arthritis of the knee as candidates for surgery are, in fact, good candidates for a partial knee replacement! The third reason for limited access to the partial knee is, unfortunately, despite uni knee benefits and slightly more difficulty in performing it, insurers under-reimburse tremendously for uni knee even more than for total knee.
We have noted over time that somewhere in the realm of 10% of people will be left with some discomfort in the front of the knee known as anterior knee pain. This occurs with or without resurfacing the patella. A few surgeons have specifically investigated doing the surgery without patellar surfacing. I quit resurfacing the patella back in the late 1990s based on their research showing it worked well; in fact, it does. That cuts a load of the cost off the knee replacement and cuts down on the pain, and the time for doing the surgery, and it eliminates the greatest cause of ultimate revision, that of loosening of the patellar component.
Since we have been able to eliminate in many people the need for resurfacing the patella, we only have to concern ourselves with the inner (medial) and outer (lateral) knee joint surfaces. The overwhelming majority of people coming in with arthritis of the knee and ultimately becoming candidates for joint replacement have at least an arthritic medial component. British surgeons believe that medial joint arthritis is a disease in itself- anteromedial degenerative arthritis. They have shown that most of these people will rarely go on to have arthritis in other parts of the knee. This has been borne out by the longevity of partial knee replacement in the United Kingdom and other parts of Europe. A much smaller portion of the population gets predominantly lateral, or outer, knee joint decay, which is much harder to resurface as a uni than a total knee, the fourth reason for poor uni knee utilization in the U.S.A.
It was thought that anteromedial knee arthritis was just an earlier stage and that over time, the patellofemoral and lateral compartments would essentially become rotten as well due to natural genetically-determined cartilage decline. It turns out that this really isn’t true in the majority of people unless they are morbidly obese. The minor decay signs on the x-ray or minor outer joint line tenderness have proven to not be an indication that a person must have a total as opposed to partial-knee replacement. Likewise, advanced arthritis on the undersurface of the patella does not seem to affect partial-knee replacement in the majority of people. A surgeon can perform the procedure, remove prominent bone spurs and perhaps partially denervate, killing the nerve endings going to the patella as part of the operative exposure and removal of these spurs, and completely eliminate the pain.
With the strong information showing that unicompartmental knee arthroplasty results are so good, what is the difference?
Partial knee replacement is done through a smaller incision. Routinely, it is done as an outpatient with minimal blood loss and no need for a transfusion, reduced risk of a blood clot, and, most of all, the joint mechanics don’t suffer. Because all the ligaments are allowed to remain intact, joint motion remains controlled by your normal ligaments and the joint motion remains normal rather than restricted as in a total knee replacement. Recovery is much faster, and costs and waste are reduced. In this day and age, being concerned about the environment and global warming if one believes that mankind is actually having any impact on it, etc., then obviously, unicompartmental knee replacement needs to be considered in any patient presenting with what appears to be limited degenerative arthritis in their knee.
Robotics - A Marketing Bonanza or Medical Manna
One of the first giant gimmicks that I have had to deal with over the past 30 years is the introduction of laser. Ultimately, laser has had almost no benefit anywhere in orthopaedic surgery. This has been much to the chagrin of the manufacturers. The next great gimmick has been pushing the concept of hyaluronic acid/rooster comb product for arthritis which has largely been a waste of time. The third gimmick was chondroplasty- shaving of degenerative cartilage- won’t grow back and it doesn’t help an arthritic knee.
The next has been pushing the concept of robotics hoping that expensive, computer-guided cutting jig and perfection of the cuts would improve the outcome of patients. No well-performed study to this date, and there have been a few, has been able to demonstrate improved patient outcome with the use of robotics for hip or knee replacement surgery. It increases the operative time which increases cost, and the machines are very expensive which also increases cost. Robotics are being used as a gimmick to try and draw patients in such as Fillmore County Hospital in Geneva (see tv ads on Me TV late night). A lot of surgeons jump on a bandwagon hoping to gain market share because they want to all give the public what they are asking for rather than following science and rational reasoning. This ties closely with the next gimmick, which was to push the concept of anterior hip replacement using a $100,000 Hana surgical table. Regardless of how one performs hip replacement, from the front or the back or side, the risk of dislocation the same. There are no improved outcomes from using the Hana, and the Hana table is not even necessary for doing anterior hip surgery if one wants to do it. No special table is necessary in skilled hands.
Denervation of joints has been used by select surgeons including myself for many years. This was prompted by the lack of resources that were available medically until the 1960s for dealing with arthritis. Anatomists in the 1800s outlined nerve endings to many of the joints in the body and, in fact, from the first arthritis surgery done for hips was the excision of the obturator nerve and geniculate nerve of the knee, etc. Identifying those nerves is sometimes very difficult and would give incomplete relief of pain depending on the joint involved. Joint replacement surgery is easier than the denervation of these. There is now a whole book written by A. Lee Dellon, M.D. (Joint Denervation: An Atlas of Surgical Techniques, 1st ed. 2019 Edition.), that has been published on denervation of various joints in the body including the knee. I started using it in about 1987 on the wrist.
We know that when a nerve is subjected to extremely cold temperatures, it will become inactive for a period of about three months. This has been widely used by some surgeons including myself in the 1980s on people with chronic back pain related to facet joint arthritis. I started using it on the wrist for posterior interosseous nerve denervation in about 1989. It is now being offered as an expensive service to possibly decrease pain associated with knee replacement because it is not a permanent solution to knee pain. The data is not in on where to place this since it is so expensive. If your medical team knows and uses the medicines available properly, there is not going to be a load of pain immediately after the surgery or down the road. Some people will continue to hurt to some degree for months, but of a minor magnitude. Rather than wasting money on things like cryo and robotics, the money should be directed to the surgeons who are underpaid and thus not motivated to do a partial knee replacement, which is better for the patient, because the insurers want to pay half as much for a more difficult operation. Write your congressman and state insurance regulators to get this situation improved!

Who is a candidate for knee replacement, uni or total?
A person who has painful degenerative arthritis of the knee not responding to or intolerant of medication, unable to use a cane successfully if appropriate, and otherwise healthy enough to undergo an operation under spinal or general anesthesia as determined by their internal medicine doctor. Diabetics need to have their diabetes well under control with a hemoglobin A1c, i.e., average serum glucose, of close to normal, or their risk of infection skyrockets. It has been determined that patients who undergo removal of a joint replacement because of infection are basically living the life profile of a person with cancer, very costly and has a lower life expectancy. It may be that these people are just typically less healthy, to begin with.
The cruciate ligaments, i.e., the ACL and the PCL, are important for the rotational stability of the knee. Mobile-bearing uni knees really need to have both their cruciates intact. Cemented uni knees need to have at least a PCL. For a total knee replacement, we have implants that will account for the absence of the cruciates, and in fact, many surgeons will remove both cruciates in the performance of total knee replacement, thus changing the mechanics of the knee, for ease of implantation.
Patients with inflammatory arthritis (rheumatoid) are not candidates for uni knee because the disease affects the whole joint and they have a great chance of progressing to destruction of the opposite of the knee if they originally present with partial-knee damage.
Severe deformity cannot be corrected with partial-knee replacement. Candidates require total knee replacement if deformity is to be corrected.
Both diabetes and morbid obesity increase the risk of blood clot and thus the risk of death from same as well as the risk of infection. I’m not sure if obesity increases the risk of loosening of implants. It definitely makes the surgery more difficult.
Risks
The risks of undergoing a knee joint replacement are bleeding, infection, and blood clots of the calf or upper thigh area that could migrate up to the lungs, i.e., pulmonary embolus, which can be fatal in a number of people. These risks have to be weighed against the benefit of pain relief, increased mobility, cutting down some medication that was being taken for pain and/or inflammation, and allowing those people who really want to become more active, admittedly a minority.
Generally, a joint replacement for arthritis does not improve motion substantially. In fact, most patients who undergo a total knee replacement lose motion and end up with an average of about 105 degrees of flexion, the minimum amount to properly go up and down stairs. Normal knee motion is from 0 to 135-140 degrees. Thus, there is about a 35-degree loss of knee motion in many patients related to scarring and inactivity. At the time of surgery, the surgeons clearly demonstrate tremendous motion. Habitually inactive patients allow the “new knee” to become stiff regardless of the amount of physical therapy attended. Unicompartmental knee replacement does not affect knee motion. It possibly increases it in people just by eliminating pain, but because the ligaments are allowed to remain, one is just removing arthritis on one side of the knee. Much like putting a crown on a tooth. The mechanics of the knee are not changed.
Summary and Conclusion
We have a major problem with overeating, the resultant obesity, and a sedentary lifestyle that is in direct relationship to the increasing number of people requiring treatment for knee arthritis. There is clear evidence that most of the people coming in for knee arthritis surgery either haven’t met the criteria, i.e., haven’t taken enough of the right medication to satisfy failure of the medication and are unwilling to use a cane or lose enough weight, which could help a lot of them get by for a long time. Ultimately, a very large percentage of the patients who are getting total knee replacement could actually get as good or better results with a partial-knee replacement with less side effects, possibly better pain relief, and equal longevity that will last just as long but with lower risk. The main impediment to getting this treatment is actually inadequate reimbursement by the nearsighted insurance companies.