

Tendon Injury In The Hand
Introduction
Hand surgery as a specialty has evolved in the 1930’s and 1940’s in response to wartime injury. Hand surgery is an art that is different from other areas of surgery. The anatomy of the hand is more complex than anywhere else in the body. Nowhere else are so many structures acting in harmony to produce motion, sensibility, and motion.
There are about:
- 27 bones
- 31 tendons
- 15 nerves
- 15 muscles
Tendons are tough, fibrous, white bands or cords connecting muscle to bone. Tendons have enormous strength to resist rupture. They allow us to move our joints.
Ligaments are the bands joining bone to bone to stabilize the joints. Thus, tendons move while ligaments, aside from stretching to allow joint motion, are rather immobile. Tendons generally act upon (cause motion) all joints they cross over.
Injuries
Injury to a tendon can be catastrophic. After a tendon is cut (laceration) end-to-end repair is necessary to regain lost motion. Best results are obtained with tendon repair occurring within days to a few weeks of injury at most. Delay in response allows muscle contracture (shrinkage), scarring, and stiffness of the joints normally acted upon by the muscle-tendon unit.
Even with prompt, meticulous tendon repairs, a good result is not guaranteed. Ragged wounds, (gunshot, crush, etc.) are less apt to heal without heavy scarring and stiffness than clean, neat wounds from a sharp object. Only rarely does a tendon rupture spontaneously, and then usually it is in association with prominent bone rubbing it or rheumatoid disease eroding into it.
So the greater the tissue damage, the greater the swelling and scarring with resultant stiffness.
Additionally, a delicate balance exists between tendon gliding and joint motion. Often a tendon will have to move only a few millimeters (less than ¼ to ½ inches) to affect the majority of joint motion.
Tendon Repair Surgery
The surgeon’s task is to identify the injured structure, plan the method and best order of repair (bone first, tendon next, and nerve and/or artery last) and then execute a meticulous repair.
Surgical technique is important, but really the greatest variable is the cooperation of the injured patient in adhering to the postoperative directions. Most of the time tendons heal best if we allow some limited gliding without resistance, i.e. passive range of motion (PROM). Active range of motion (AROM) puts too much tension on many repairs and may result in significant gap formation (separation of cut tendon ends), thus reducing joint motion when healed. Rupture of the repair and thus failure to benefit from the surgery and prolonged impairment (loss of function) may occur even with careful attention to following directions, fortunately, less than 2-5% of repaired flexor tendons will rupture.
Extensor tendons on the top of the hand are less prone to scar adhesion than flexors. Unlike the flexor tendon, the extensors do not lie in a tight channel, but rather glide beneath the subcutaneous skin.
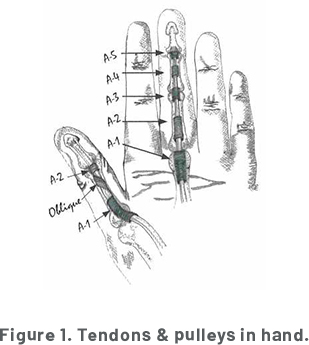
Making tendon injury and repair more difficult is the criss-cross arrangement of the two-flexor tendons in each finger.
The short, superficial flexor (FDS) bends the PIP joint while the FDP bends the DIP in addition to assisting with bending the PIP.
To prevent scar adherence and resultant loss of motion and to strengthen the repair site, specific exercises including splints to maintain optimal finger posture are essential.
Tendon Surgery Post-Operative Care
Complying with post-operative instructions is critical if you want to experience a good result.
Late reconstruction is more difficult, more time-consuming, and less successful than primary repair at the time of injury.
Usually, restricted motion in a protective splint is recommended for about 6 weeks. After splint removal, only light use of one’s hand is usually advisable for an additional 4-6 weeks while further repair site strength and motion are obtained.
Motion is also important to maintain the elasticity of ligaments. If a joint is not moved enough the ligament will tighten up preventing motion even if tendon gliding is otherwise possible.
Skin stitches are usually removed at 10-14 days post-op. The skin healing occurs much faster than tendons heal. At 4 weeks, a flexor tendon is just beginning to heal (much like a construction crew getting organized to begin a building project).
Our lives may be severely affected by poorly functioning, stiff, or numb fingers or thumbs.
PROTECT YOUR ASSETS! BE CAREFUL WITH YOUR HANDS!